
Investigating the Role of Monoamine Oxidase Inhibitors in the Treatment of Major Depressive Disorder
Monoamine Oxidase and Depression | Cal Westbury
This literature review focuses on the monoamine oxidase inhibitor (MAOI) family by considering past research to provide information on the pharmacology of MAOIs, their mechanism of action, and the role they have in treating major depressive disorders. MAOIs work by disabling monoamine oxidase, an enzyme that breaks down neurotransmitters. This class has been used for decades but is overshadowed by selective serotonin reuptake inhibitors due to their similar effect and higher therapeutic index. Their uniqueness makes MAOIs a viable and effective option for patients with treatment-resistant depression who are finding other antidepressants ineffective.
Pathophysiology of Depression
Depression is a mental disorder that is characterised by a lack of motivation and excitement, a lowered self-esteem, a drastically low mood, and aversion to most social activities. Patients suffering from clinical depression, also known as major depressive disorder (MDD), may experience physical symptoms such as fatigue, insomnia, headaches, and nausea. The pathophysiology of depression is widely discussed as numerous theories hold potential. The leading theory revolves around a deficiency in a patient’s monoaminergic system. This system regulates and circulates monoamine neurotransmitters, which are characterised on a molecular level by an amino group bound to an aromatic ring by a dual-carbon chain. Examples of these neurotransmitters include dopamine, serotonin, and norepinephrine, some of the critical components in neuromodulation and mood function. As such, treatment options were often therapeutics that would release or reintroduce monoamine neurotransmitters, such as monoamine oxidase inhibitors (MAOIs). This class of antidepressants consistently and reliably treated depressive symptoms in MDD and treatment-resistant depression (TRD) before being phased out in place of serotonin reuptake inhibitors (SSRIs).
Dopamine
Dopamine is a monoamine neurotransmitter primarily used in the modulation of motivational salience, acting to moderate reward and incentive responses. It is the main component of several neural pathways, one of which is the reward-motivation behaviour pathway. Anticipation of a reward triggers the release of dopamine, which reinforces that activity. Due to this, many drugs that increase the abundance or availability of dopamine in the brain are highly addictive. For example, cocaine has been found to inhibit reuptake of monoamine neurotransmitters, primarily dopamine and norepinephrine [1]. This quickly builds an addiction through the repeated supersaturation of dopamine, causing the reward centres to repeat the activity. The two primary subtypes of dopamine receptors, dubbed D1 and D2, contain receptors D1 through D5. All five subtypes of dopamine receptors are G-protein coupled receptors that are composed of the characteristic seven transmembrane regions and form the dopamine binding site (Figure 1). A decrease in the availability of monoamines can cause a significant reduction in the level of dopamine in the brain; damaged dopamine receptors (from drug use, nerve damage, or genetics) can create an equivocal effect, as more dopamine is needed to create the normal response. Low levels of dopamine are directly linked to difficulty concentrating, tiredness, a lack of motivation, and an absence of sex drive.
Patients with depression have been found to have decreased activity in the D1 and D2 subtype receptors [2]. This can be linked to the physical symptoms patients suffering from major depressive disorder experience, such as fatigue, agitation, and restlessness, as the dopaminergic pathways are used to regulate those processes.
Serotonin
Serotonin, or 5-HT, is a monoamine neurotransmitter involved with mood, cognition, reward, and various physiological processes, including vomiting and vasoconstriction. Roughly 90% of the serotonin produced by the body is done so via enterochromaffin cells in the gastrointestinal tract, which act to regulate intestinal movements [3]. The remaining 10% of serotonin is produced in the central nervous system, mainly in the raphe nuclei. The raphe nuclei are found primarily in the brainstem, acting to modulate the release of serotonin via an autoreceptor loop [4]. The primary purpose of serotonin in research and clinical interest is to modulate mood. A majority of mood regulation comes from serotonergic projections that originate from the caudal linear nuclei, which include the nucleus raphe magnus, the raphe obscurus nucleus, the raphe pallidus nucleus, and the lateral medullary reticular formation. The caudal linear nuclei project into multiple cortical structures but mainly into the brainstem. The projections that originate from the caudal nuclei are directly associated with mood regulation; hyposerotonergic [5] and hyperserotonergic [6] states have been associated with involvement in depression. Disorders caused by serotonergic activity, whether high or low, have been observed to heavily contribute to the symptoms of MDD, including mood, cognition, sexual dysfunction, and suicidality [7]. This has been linked to a potential cause of MDD - a decreased size of the locus coeruleus, a nucleus in the pons of the brainstem. The locus coeruleus, not only adjacent to the caudal linear nuclei but also near identical in function and structure, corresponds to the modulation of mood. More indication of a link is the apparent efficacy of drugs that work on this nucleus, including serotonin-norepinephrine reuptake inhibitors (SNRIs) like venlafaxine, norepinephrine-dopamine reuptake inhibitors (NDRIs) like bupropion, and norepinephrine reuptake inhibitors (NR) like atomoxetine.
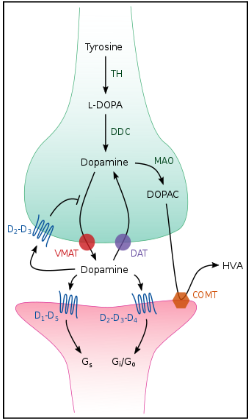
Figure 1: Dopamine receptor and processes.
Norepinephrine
Norepinephrine is a monoamine neurotransmitter in the catecholamine family. The key function of norepinephrine is to activate the brain and body, preparing them for action. In the brain, norepinephrine increases alertness, memory, and focus. It also acts to increase heart rate, blood flow to skeletal muscle, and the release of glucose stores for energy. Norepinephrine that affects the brain is produced by small nuclei located in the pons. Many of these nuclei remain mostly unstudied but are commonly associated with the production and release of serotonin. The locus coeruleus in the pons is the primary location for norepinephrine synthesis in the brain. A damaged or undeveloped locus coeruleus has been proposed as a theoretical cause of MDD due to the unavailability of norepinephrine [1]. A huge variety of both medicinal and recreational drugs work by altering the noradrenergic system in either agonistic or antagonistic ways. Most stimulant drugs work by synergising, potentiating, or activating noradrenergic pathways, creating a strong agonistic effect. This agonistic action triggers a cascade of neurophysiological signalling that results in increased blood pressure, heart rate, and vigilance, as well as reducing many gastrointestinal processes [1]. Recreational drugs, such as cocaine, work by inhibiting the reuptake of norepinephrine and dopamine, with a slight inhibitory action on serotonergic reuptake. This causes a stimulant action and a moderate antidepressant effect. The most commonly used stimulants in a clinical setting are in the amphetamine family, which act as dopamine and norepinephrine analogues and reuptake inhibitors throughout the body.
The links between each monoamine, both in isolation and in unison, have led researchers to consider the depletion of monoamines, primarily and most importantly serotonin, as the cause of MDD. The rationale behind this theory lies in the observed correlation between the acute depletion of tryptophan, a foundational a-amino acid responsible for the biosynthesis of multiple neurotransmitters, primarily serotonin (5-hydroxytryptamine). When the inadequacy of tryptophan occurs, a cascading effect follows, leading to decreased amounts of serotonin and melatonin, which is a direct cause of depression [8]. Current treatments for MDD revolve around the reintroduction or release of monoamines, particularly serotonin. The most common class of antidepressants, SSRIs, act to reduce the amount of serotonin reabsorbed by the brain. The process of reuptake involves signals in the postsynaptic cells of a recipient receptor when a neurotransmitter is present in the synaptic gap. A signal is sent via a chemical synapse and monoamine transporters are released, reabsorbing up to 90% of the neurotransmitters between the synapses back into the presynaptic cell. By interrupting the postsynaptic messaging to the sending cell, the reuptake cycle is preemptively halted (Figure 2). This results in an increase of serotonin in the synaptic gap, increasing the amount available to the receptor sites and creating repeated agonistic action on the receptors. SSRIs work slowly, taking weeks to evoke an effect on the patient’s level of serotonin. As such, the characteristically slow-forming psychiatric effects of the drugs are attributed to this [9]. In contrast, MAOIs are often able to evoke a therapeutic psychiatric effect much faster than SSRIs, simply due to their mechanism of action and pharmacodynamic properties.

Figure 2: Serotonin receptor, including the mechanism of SSRIs.
Pharmacology of MAOIs
MAOIs are an early class of antidepressants that function by inhibiting monoamine oxidase (MAO): MAO-A, MAO-B, or both. MAO is an enzyme that catalyses oxidation, hence the breakdown of monoamine neurotransmitters like serotonin, by using oxygen to cleave off the amine group of the molecules. They regulate the levels of monoamines in the body, moderating sympathetic nervous system functions and preventing excess levels. Grouped in the flavin-containing amine oxidoreductase family, MAO also works to reduce intracellular levels of trace amines and neurotoxins, and plays a key role in the modulation of mood and upkeep of certain cognitive functions. It has been found that in untreated patients diagnosed with MDD, MAO-A levels are elevated on average by 34% [11]. Through the selective inhibition of these enzymes, there is a repopulation of monoamine neurotransmitters, leading to an improvement in the symptoms of depression. A common selective MAOI is moclobemide, a selective and reversible inhibitor of MAO-A (RIMA). Moclobemide, along with other RIMAs, is uncommonly prescribed due to concerns about its influence on monoamine levels. Moclobemide’s mechanism of action counteracts the raised levels of MAO-A in patients diagnosed with depression [11]. There is clear evidence that MAO-A is localised to a high degree in the locus coeruleus, within the noradrenergic neurons [12]. Unlike non-selective and irreversible MAO-A inhibitors, moclobemide does not cause elevated blood pressure in combination with other amines, such as from foods that contain tyramine, or pressor amine drugs used to control hypotension like methoxamine. This means that moclobemide, from a purely clinical analysis, is safer to prescribe to patients, particularly those with which the provider has concerns over tolerance. Moclobemide’s efficacy is shown in numerous studies, with one notable description, “Compared with SSRIs, moclobemide has a similar overall tolerability, although it tends to cause fewer gastrointestinal effects than the SSRIs and has not been reported to interfere with sexual function. In summary, recent data which confirm and extend its comparative therapeutic efficacy and low potential for adverse effects have established moclobemide as an effective treatment in depressive disorders.” [13]. This comment is backed by Figure 3 which recognises moclobemide as a drug that does not have the characteristic low tolerability of other MAOIs, and does not produce the tyramine-associated pressor effects as others do. In the treatment of elderly patients with MDD, moclobemide is identified not only as more efficacious on the Hamilton depression rating scale (HDRS) than placebos, but also as producing fewer adverse effects than the industry-favoured SSRI family.

Figure 3: Comparative results of MAOI Adverse effects against placebo [14].
Similar in theory to moclobemide, selegiline is a selective and irreversible inhibitor of MAO-B. Unlike moclobemide, which is typically indicated for the treatment of MDD and social anxiety disorder [12], selegiline is more commonly prescribed for adjunct treatment of Parkinson’s disease, with evidence showing efficacy following initial treatment with levodopa [15]. Selegiline binds covalently to MAO-B, presumably producing effects by preventing the oxidation of dopamine, thus increasing its availability. The theorised neuroprotective properties of selegiline likely come from the inadvertent prevention of free oxygen radicals near neurons that are produced by MAO-B’s action. High doses of selegiline has shown to inhibit MAO-A, leading researchers to question the drug’s selective status. Selegiline lacks the rapid gastrointestinal absorption that makes moclobemide a viable oral drug, leading to the use of transdermal patches for administering selegiline in the USA. This method avoids the inhibition of MAO enzymes in the gastrointestinal and hepatic regions, preventing the risk of food-derived tyramine reaching adverse levels [16].
At median dosages, typically 6-12 mg/day, the transdermal delivery system shows efficacy in the treatment of depression and does not impose dietary restrictions on the patient’s tyramine intake. In higher doses of 9 mg+/day, used in severe cases of depression, restriction of dietary tyramine intake is recommended, as tolerance can wane at larger doses [16]. In contrast to oral doses, transdermal application of selegiline indicates a 50-fold increase in exposure compared to previous oral alternatives, while lowering exposure to metabolites by over 70% [17]. Via the alternative administration and avoidance of tyramine exposure, or ‘cheese reaction’, the adverse effects of selegiline are as expected of antidepressants, regardless of class. The most common adverse effects were application site reaction, dyspepsia, and dry mouth. In placebo trials, 7.1% of patients receiving selegiline discontinued usage of the transdermal patch, compared to 3.6% of patients receiving placebo. In all cases, application site reaction was the only adverse reaction causing the discontinuation of the treatment.
A case report on the efficacy of selegiline on a single patient with stage 5 TRD details the effectiveness of MAOI drugs in the treatment of specific and resistant depression. The patient’s record included four ineffective or intolerable antidepressants, and electroconvulsive therapy which yielded only a temporary result. The patient had previously been treated with various classes of antidepressants; most notable was 40mg/day of paroxetine, the recommended maximum dose. Paroxetine shows the most potency of the SSRI family, so its inefficiency is further evidence of the patient’s resistance to typical antidepressants. [18]. Also notable is the repeated application of tricyclic antidepressants (TCAs), an archaic family of antidepressants typically indicated for lower-severity depression. The patient received TCAs a total of three times, being prescribed imipramine, amitriptyline, and clomipramine, all with minimal efficacy.
Following the shortfallings of tricyclic antidepressants, the patient was prescribed 10mg/day of transdermal selegiline. During the 20-week observed therapy, the patient’s HDRS score dropped substantially, first to 9 points at week 8, and then to 4 points at week 20. Blood dopamine levels also rose noticeably following treatment, evidencing selegiline’s potential dopaminergic action and therapeutic benefit [19]. The patient’s glucose metabolism showed a marked increase during and following selegiline treatment. Using [18F]-fluorodeoxyglucose positron emission tomography, the positive change in the patient’s glucose metabolism within the bilateral basal ganglia is visible (indicated with red arrows), as is the decreased glucose metabolism in the occipital lobe (indicated with white arrows). The pictured FDG-PET depicted in Figure 4 includes a scan done prior to selegiline treatment (Figure 4A) and another performed at week 20 when the patient’s HDRS score had decreased to 4 points (Figure 4B) [19].

Figure 4: FDG-PET of a TRD Patient before (A) and after (B) selegiline treatment [19].
The nature of both moclobemide and selegiline in the treatment of MDD indicates that both MAO-A and MAO-B inhibitors can offer effective, tolerable, and safe alternatives to the industry-dominating SSRI drugs that commonly fail to improve a patient’s mental state while creating adverse effects. The apprehension towards MAOIs for their intolerability and risk of tyramine exposure is now academically unacceptable as research steadily shows how the use of MAOIs is efficacious and should be more closely tied to the treatment of MDD.
Unlike the characteristically selective drugs mentioned previously, phenelzine is a non-selective and irreversible hydrazine MAO inhibitor. The hydrazine class of MAOI is characterised by the hydrazine (N2H4) group found in the formula of each. Hydrazine itself is considered highly toxic, and as such, many hydrazine MAOIs feature a risk of toxicity, particularly hepatotoxicity via hepatic metabolism [20]. Unlike other, now withdrawn, hydrazine antidepressants, phenelzine is clinically and medically acceptable for use and remains approved by the FDA. Phenelzine, being non-selective, is marginally more likely to produce a tyramine overexposure reaction, causing hypertension and headaches. That, in combination with its oral route of administration, in contrast to selegiline’s transdermal approach, means more gastrointestinal and hepatic MAO inhibition, leading to a greater risk of tyramine reactions. The key benefits of phenelzine that justify the slight risk of a non-selective drug and its potential off-target binding come from the drug’s unique metabolism and pharmacodynamics.

Figure 5: The structure of phenelzine (left) vs the structure of amphetamine (right).
The pharmacodynamics of phenelzine are, in essence, distinctively strange. The elimination of MAO leads to an increase in specialised brain amines, such as 2-phenylethylamine, which have been shown to greatly increase the availability of catecholamines and serotonergic activity in nerve endings via action on uptake and release [21]. Phenelzine also elevates the levels of gamma-aminobutyric acid (GABA) and alanine (ALA) in the brain, both of which show efficacy in improving mental state and treating neurotic, atypical, and major depression [22]. Phenelzine’s uniqueness can be partially attributed to its structure, some aspects of which it shares with amphetamine, explaining certain dopaminergic and serotonergic activity present in phenelzine’s pharmacodynamics (Figure 5).
The definitive feature of phenelzine, which remains striking, is its metabolites. The most important of these is phenylethylidenehydrazine, a potent inhibitor of GABA transaminase, which is thought to improve the therapeutic effects of phenelzine and contribute to its anxiolytic properties [23]. As the primary inhibitor messenger in the brain, the consequential elevation of GABA is vital for the effective treatment of anxiety and depression that is attributed to phenelzine. Through an intrinsic mechanism, phenelzine is reported to competitively inhibit tyrosine aminotransferase and dopamine β-hydroxylase, allowing for not only elevation of typical monoamine molecules such as dopamine, but also the precursor amino acids that are theorised to contribute to the treatment of MDD [21].
The greatest concern over the usage of MAOIs (not just phenelzine), stems from a predictable and common reaction to the repeated usage of MAOIs, typically seen in non-selective members of the family. Despite the therapeutic effects of inhibiting MAO, risks and adverse effects come with them. By eliminating a vital inhibitory enzyme, other monoamines that would usually be held in check become elevated, and exposure to them can lead to negative symptoms. The primary candidate for these reactions is tyramine. Tyramine is a naturally occurring trace amine that forms commonly from the decarboxylation of tyrosine during natural fermenting or ageing processes [24]. Foods that contain high levels of tyramine include aged dairy products, such as cheddar or chocolate. While tyramine may seem unassuming in the presence of metabolising enzymes like MAO from a clinical standpoint, its effects can be significant in the absence of such enzymes. Tyramine can displace stored monoamines from synaptic vesicles, creating an imbalance in blood pressure and consequently a hypertensive crisis and headaches. Delving deeper, tyramine exerts a vasopressor effect due to its action as a sympathomimetic agent. Tyramine also affects the norepinephrine transporter, leading to an increase in the release of norepinephrine. This leads to a vasoconstricting effect, producing an increase in blood pressure and heart rate [25]. Though reported in phenelzine, the most common cause of the tyramine reaction or ‘cheese reaction’ was produced by the non-hydrazine, non-selective MAOI, tranylcypromine [26]. The concerns of hypertensive crisis and the risks of headaches that come with it have driven healthcare providers to avoid the prescription of MAOIs, particularly non-selective hydrazine MAOIs, which, with the exception of tranylcypromine, most commonly produces the dreaded ‘cheese reaction’ [27]. It is also of note that both compounds bind irreversibly to the peptide chains within flavine-adenosine-diphosphate, a coenzyme of both MAO-A and MAO-B. Due to the antagonistic action and permanent peptide binding, biosynthesis of new enzymes is required to restore the action of the MAO enzymes.
Exploring potential measures to bypass toxicity
Modern research has improved the viability and tolerance of MAOIs by replacing traditional non-selective irreversible MAOIs with alternatives like RIMAs. RIMAs are more tolerable, do not provoke a tyramine reaction, and do not require more novel routes of administration, like the transdermal patches used to administer selegiline. By researching such means and by controlling dosing regimens in a manner that prevents the commonplace dietary restrictions that come with MAOI prescription, MOAIs can provide greater efficacy in the treatment of atypical depressive disorders which most primary antidepressants are not specialised for. A review of research on the transdermal application of selegiline has yielded conclusions that the drug’s favourable collection of side effects (in contrast to alternative treatments for severe or atypical depression), as well as its lack of dietary restrictions for those on controlled doses, allows selegiline to not only remain viable but also offer greater and more consistent exposure to the parent compound, with minimal loss of compound from first-pass metabolism and digestion [28].
The trait that is shared between all efficacious MAOIs, except for the estranged child phenelzine, is selectivity. Selectivity, primarily in the inhibitors of MAO-A, provides the increase in serotonergic levels and general mood that classes them as effective antidepressants. MAO-A primarily deaminates serotonin and norepinephrine, both of which are considered key in the pathophysiology of depression [29]. In the realm of clinical neuropharmacology, certain factors are notable. Selective inhibitors of MAO-A are nearly constantly reversible, falling into the RIMA family, while inhibitors of the MAO-B selective antagonists are only available in an irreversible form. Each subtype, or selectivity, is more specifically honed for contrasting dynamic actions. This, in turn, means that each has its strategies for reducing adverse effects and minimising the risks and severity of toxicity. The management of toxicity developed in today’s MAOI market has been the result of decades of cultivation from the first-generation non-selective family, most of which held the threat of a low therapeutic index. While there have been marked improvements, primarily with the development of the transdermal delivery of selegiline, the risks and unpredictability of non-selective MAOIs remain present. Should research be furthered into the deep possibilities of MAOIs, a select few drugs would yield preference in both tolerance and future development potential. Selegiline’s transdermal application may be explored with alternative MAOIs; the most likely candidates would be the non-selective subfamily. The landscape of modern treatment of MDD, particularly in patients resistant to previous therapies, would be fundamentally transformed, given the implementation of a countermeasure for the ever-present risk of tyramine reaction in non-selective MAOIs. The feared and sometimes vilified non-selective MAOIs, such as tranylcypromine and phenelzine, could become viable and useful, garnering a place in the growing roster of drugs against depression.
Role in depression
From a pragmatic and realistic standpoint, the current climate of treatment options for MDD shows no likelihood of a sudden turn towards the MAOIs that, though approved for treatment, have been gathering dust. There are clear reasons for this. SSRIs offer the most widely tested and reliable measure of efficacy and safety out of the class. Due to the more understood mechanisms, more specified targets, and greater potential for combination use, SSRIs are traditionally used for mild to moderate depression. Flaws arise only in nonstandard cases, such as in TRD or atypical depression. In these cases, combination targeting is shown to work better. In a study observing the HDRS of inpatients with major depression treated only with desipramine, a TCA that has primarily noradrenergic action, versus the HDRS of patients treated with both desipramine and fluoxetine, a common SSRI used in the treatment of depression and social anxiety. Patients treated with the combined therapy underwent faster improvement of symptoms; two drugs in synergy showed greater efficacy, possibly attributed to the inhibited metabolism of desipramine in the presence of fluoxetine [30]. When treated by the dual drugs, which exerted both a serotonergic and noradrenergic action, the patients had a mean decrease in HDRS score of 42% one week after treatment began, while the patients given only desipramine had a mean decrease of 20% at the same timestamp, as seen in Figure 6 (p=0.007) [31]. With another week of treatment, the mean change in the score of the dual-treatment patients was 60%, while that of the single-treatment patients was 30% (p=0.001).
After the study, following 4 weeks total of treatment, 71% of the patients receiving serotonergic and noradrenergic action had a positive change in HDRS score of 75% or greater, with the final score being below 7, showing remission [31]. This study indirectly shows the therapeutic advantage of broad-scope treatments that act upon more than one neurotransmitter, furthering the evidence that MAOIs have a niche in the treatment of depression. To claim that MAOIs could replace or even complement most current first-line treatments would be uneducated or baseless. However, due to the evidence shown in recent research, it is clear that MAOIs have an irrefutable niche in the psychiatric treatment of depression, particularly in cases of TRD. While MAOIs are far from novel, and further from young, research is still needed to improve the drug family as a whole for general use. This class of antidepressants, typically intolerable to a degree, contains some gems. Selegiline and moclobemide hold genuine potential for the improvement of the treatment of depression in both efficacy and more importantly in how they affect the patient’s experience. Without dietary restrictions or the risk of hypertensive crises, which is already a milestone reached by low-dose selegiline, MAOIs pose more mild side effects than SSRIs and have equal or usually greater efficacy [32].

Figure 6: Comparison of single treatment therapy vs mixed treatment therapy & the change in HAM-D/HDRS Score. [31]
Recommendations
In typical psychiatric settings, with traditional presentations of MDD, it is unlikely and unwise to prescribe MAOIs as a first or second-line treatment. Though those treatments may successfully control the symptoms of some patients, for others they serve more as measures of a patient’s tolerance and needs as a whole. Should a patient’s HDRS remain unchanged following 10 or more weeks of daily use of SSRIs or select SNRIs like venlafaxine, the patient’s depression should be considered to have aspects of treatment resistance. It is at this point that MAOI therapy should be indicated. In studies on early and advanced-stage TRD, responses to therapy were tested with the Clinical Global Impressions Change Scale (CGI/C). A total of 75% of the 59 participants had a CGI/C score of at most 3, feeling “better”, while 56% of the participants had a score of 1 (“very much better”) or 2 (“much better”). The study showed the importance of early diagnosis of TRD, as 32.5% of early TRD patients reach a CGI/C score of 1, against the 12.1% of advanced TRD patients that did (p=0.04) [33]. The efficacy and long-term improvements of TRD patient symptoms that are shown in studies done with MAOIs establish a clear role for the family in use against depression. In my recommendation, a patient exhibiting the potential of TRD should be offered a trial on either transdermal selegiline (6 mg/day) or oral route moclobemide (150 mg, twice a day), with the prescriber’s discretion affecting the choice of selectivity. It is not necessary to force these potentially intolerable drugs into the market circulation of modern psychiatry. Rather, it is important to recognise the niche of these drugs in the reliable and efficacious treatment of depression. Phenelzine, the “elephant in the room” of all conversations about MAOIs, should be considered cautiously. In comparative studies, the non-selective MAOIs show the greatest efficacy and the fastest onset of effect out of most, if not all, antidepressants; however, the blatant downside is the risk of tyramine exposure, necessitating dietary restriction. Both phenelzine and tranylcypromine have earned themselves a place in the treatment of depression, though perhaps after a MAOI trial. SSRIs should remain the primary treatment, as though the resurrection of MAOI therapy could hold promise, the risks and archaic nature of the drug family leave it more suited for specialised usage. In a single reflective statement, MAOIs are fascinating, powerful antidepressants that not only hold potential to aid TRD patients unlike any common modern therapies but could also link to the direct cause of clinical depression, in consideration of the role of MAO in the appearance of depressive symptoms. The possible connection between neurotransmitter depletion and major depression, and hence the plausible link to the genetic profile of depression - specifically the polymorphisms of the MAO promoter regions - and the faint chance of a genetic therapy for depression, deserve both attention and research.
Conclusion
Ultimately, the significance of antidepressants and their evolution is undeniable, regardless of the current industry standards. While this literature review aimed to neatly define the niche of MAOI therapy and highlight their importance in TRD, it is vital to stress the need for further research and trial MAOIs. To quote Hippocrates, the father of medicine, “That which is used - develops. That which is not used wastes away.” The evidence of the efficacy, and at the very least potential, of the MAOI family lies nestled under decades of SSRIs and now-irrelevant research on the presently avoidable tyramine reaction that caused the whole of psychiatry to abandon MAOIs. The future of neuroscience, psychiatry, and psychology together could fundamentally change should science delve into the enigma that is MAO, and how MAOIs can help us generate new ideas and new ways to treat depression.
[1] Ritter J, Flower RJ, Henderson G, Loke YK, MacEwan DJ, Rang HP (2020). Rang and Dale’s pharmacology (Ninth ed.).
[2] Belujon, P., & Grace, A. A. (2017). dopamine System Dysregulation in Major Depressive Disorders. The international journal of neuropsychopharmacology, 20(12), 1036–1046. https://doi.org/10.1093/ijnp/pyx056
[3] Berger, M., Gray, J. A., & Roth, B. L. (2009). The expanded biology of serotonin. Annual review of medicine, 60, 355–366. https://doi.org/10.1146/annurev.med.60.042307.110802
[4] Siegel, G. J., Agranoff, B. W., Albers, R. W., Fisher, S. K., & Uhler, M. D. (1999). Basic Neurochemistry - Ch. 5. NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK20385/
[5] Hensler JG. (2009). “Serotonin in Mode and Emotions”. In Müller CP, Jacobs BL (eds.). Handbook of the behavioural neurobiology of serotonin.
[6] Andrews PW, Bharwani A, Lee KR, et al. (2015). “Is serotonin an upper or a downer? The evolution of the serotonergic system and its role in depression and the antidepressant response”.
[7] Lucki, I. (1998). The spectrum of behaviours influenced by serotonin. Biological Psychiatry, 44(3), 151–162. https://doi.org/10.1016/S0006-3223(98)00139-5
[8] Fernstrom J. D. (1983). Role of precursor availability in control of monoamine biosynthesis in brain. Physiological reviews, 63(2), 484–546. https://doi.org/10.1152/physrev.1983.63.2.484
[9] O’Brien, F. E., O’Connor, R. M., Clarke, G., Dinan, T. G., Griffin, B. T., & Cryan, J. F. (2013). P-glycoprotein inhibition increases the brain distribution and antidepressant-like activity of escitalopram in rodents. Neuropsychopharmacology : Official Publication of the American College of Neuropsychopharmacology, 38(11), 2209–2219. https://doi.org/10.1038/npp.2013.120
[10] Tsugeno, Y., & Ito, A. (1997). A key amino acid responsible for substrate selectivity of monoamine oxidase A and B. The Journal of biological chemistry, 272(22), 14033–14036. https://doi.org/10.1074/jbc.272.22.14033
[11] Meyer, J. H., Ginovart, N., Boovariwala, A., Sagrati, S., Hussey, D., Garcia, A., Young, T., Praschak-Rieder, N., Wilson, A. A., & Houle, S. (2006). Elevated monoamine oxidase a levels in the brain: an explanation for the monoamine imbalance of major depression. Archives of general psychiatry, 63(11), 1209–1216. https://doi.org/10.1001/archpsyc.63.11.1209
[12] Bonnet U. (2003). Moclobemide: therapeutic use and clinical studies. CNS drug reviews, 9(1), 97–140. https://doi.org/10.1111/j.1527-3458.2003.tb00245.x
[13] Fulton, B., & Benfield, P. (1996). Moclobemide. An update of its pharmacological properties and therapeutic use. Drugs, 52(3), 450–474. https://doi.org/10.2165/00003495-199652030-00013
[14] Amrein, R., Stabl, M., Henauer, S., Affolter, E., & Jonkanski, I. (1997). Efficacy and tolerability of moclobemide in comparison with placebo, tricyclic antidepressants, and selective serotonin reuptake inhibitors in elderly depressed patients: a clinical overview. Canadian journal of psychiatry. Revue canadienne de psychiatrie, 42(10), 1043–1050. https://doi.org/10.1177/070674379704201005
[15] Pringsheim, T., Day, G. S., Smith, D. B., Rae-Grant, A., Licking, N., Armstrong, M. J., de Bie, R. M. A., Roze, E., Miyasaki, J. M., Hauser, R. A., Espay, A. J., Martello, J. P., Gurwell, J. A., Billinghurst, L., Sullivan, K., Fitts, M. S., Cothros, N., Hall, D. A., Rafferty, M., Hagerbrant, L., ... Guideline Subcommittee of the AAN (2021). Dopaminergic Therapy for Motor Symptoms in Early Parkinson Disease Practice Guideline Summary: A Report of the AAN Guideline Subcommittee. Neurology, 97(20), 942–957. https://doi.org/10.1212/WNL.0000000000012868
[16] Lee, K. C., & Chen, J. J. (2007). Transdermal selegiline for the treatment of major depressive disorder. Neuropsychiatric disease and treatment, 3(5), 527–537.
[17] Barrett, J. S., Hochadel, T. J., Morales, R. J., Rohatagi, S., DeWitt, K. E., Watson, S. K., & DiSanto, A. R. (1996). Pharmacokinetics and safety of a selegiline transdermal system relative to single-dose oral administration in the elderly. American journal of therapeutics, 3(10), 688–698. https://doi.org/10.1097/00045391-199610000-00004
[18] Mozayani, A., & Raymon, L. (2011). Handbook of drug interactions: a clinical and forensic guide. Springer. p. 216.
[19] Kitaichi, Y., Inoue, T., Mitsui, N., Nakagawa, S., Kameyama, R., Hayashishita, Y., Shiga, T., Kusumi, I., & Koyama, T. (2013). Selegiline remarkably improved stage 5 treatment-resistant major depressive disorder: a case report. Neuropsychiatric disease and treatment,9, 1591–1594. https://doi.org/10.2147/NDT.S49261
[20] Lopez-Munoz, F., & Alamo, C. (2013, April 14). Bentham Science Publishers. Archive.Ph. https://archive.ph/20130414065844/http://www.bentham-direct.org/pages/content.php CPD/2009/00000015/00000014/0002B.SGM
[21] Baker, G. B., Coutts, R. T., McKenna, K. F., & Sherry-McKenna, R. L. (1992). Insights into the mechanisms of action of the MAO inhibitors phenelzine and tranylcypromine: a review. Journal of psychiatry & neuroscience : JPN, 17(5), 206–214.
[22] Todd, K. G., & Baker, G. B. (2008). Neurochemical effects of the monoamine oxidase inhibitor phenelzine on brain GABA and alanine: A comparison with vigabatrin. Journal of pharmacy & pharmaceutical sciences : a publication of the Canadian Society for Pharmaceutical Sciences, Societe canadienne des sciences pharmaceutiques, 11(2), 14s–21s. https://doi.org/10.18433/j34s38
[23] Parent, M. B., Master, S., Kashlub, S., & Baker, G. B. (2002). Effects of the antidepressant/antipanic drug phenelzine and its putative metabolite phenylethylidenehydrazine on extracellular gamma-aminobutyric acid levels in the striatum. Biochemical pharmacology, 63(1), 57–64. https://doi.org/10.1016/s0006-2952(01)00856-5
[24] National Center for Biotechnology Information (2024). PubChem Compound Summary for CID 5610, Tyramine. Retrieved February 27, 2024 from https://pubchem.ncbi.nlm.nih.gov/compound/Tyramine.
[25] Raiteri, M., Del Carmine, R., Bertollini, A., & Levi, G. (1977). Effect of sympathomimetic amines on the synaptosomal transport of noradrenaline, dopamine and 5-hydroxytryptamine. European journal of pharmacology,41(2), 133–143. https://doi.org/10.1016/0014-2999(77)90202-3
[26] Ogbuagu Emmanuel, O., Uloaku, O., & Offiah, A.U. (2020). Tyramine Induced Hypertension (TIH)-A review. Journal of Medical Investigation and Practice, 11(2), 27–31.
[27] Lavian, G., Finberg, J. P., & Youdim, M. B. (1993). The advent of a new generation of monoamine oxidase inhibitor antidepressants: pharmacologic studies with moclobemide and brofaromine. Clinical neuropharmacology, 16 Suppl 2, S1–S7.
[28] Culpepper, L., & Kovalick, L. J. (2008). A review of the literature on the selegiline transdermal system: an effective and well-tolerated monoamine oxidase inhibitor for the treatment of depression. Primary care companion to the Journal of clinical psychiatry, 10(1), 25–30. https://doi.org/10.4088/pcc.v10n0105
[29] Yamada, M., & Yasuhara, H. (2004). Clinical pharmacology of MAO inhibitors: safety and future. Neurotoxicology, 25(1-2), 215–221. https://doi.org/10.1016/S0161-813X(03)00097-4
[30] Wilens, T. E., Biederman, J., Baldessarini, R. J., McDermott, S. P., Puopolo, P. R., & Flood, J. G. (1992). Fluoxetine inhibits desipramine metabolism. Archives of general psychiatry, 49(9), 752. https://doi. org/10.1001/archpsyc.1992.01820090080014
[31] Nelson, J. C., Mazure, C. M., Bowers, M. B., Jr, & Jatlow, P. I. (1991). A preliminary, open study of the combination of fluoxetine and desipramine for rapid treatment of major depression. Archives of general psychiatry, 48(4), 303–307. https://doi.org/10.1001/archpsyc.1991.01810280019002
[32] Bodkin, J. A., & Amsterdam, J. D. (2002). Transdermal Selegiline in Major Depression: A Double-Blind, Placebo-Controlled, Parallel-Group Study in Outpatients. American Journal of Psychiatry, 159(11), 1869–1875.https://doi.org/10.1176/appi.ajp.159.11.1869
[33] Amsterdam, J. D., & Schults, J. (2005). MAOI efficacy and safety in advanced stage treatment-resistant depression—A retrospective study. Journal of Affective Disorders, 89(1–3), 183–188. https://doi.org/10.1016/j.jad.2005.06.011
Cal is studying a BSc (Pharmacology) degree and has hopes to do research in neuroscience. While he has an emphasis on depression, he takes a multifocal approach to study; looking at patient-specific treatments for heart failure. Outside study, Cal spends his time listening to music and writing fiction.